The Unwanted Holiday Souvenir: Heartworm
Recognising and managing heartworm as an emerging risk in travelling and imported dogs

“Have you seen any cool cases lately?” is a question we are often asked when visiting clinics. Of course, anything heart-related is cool to us (so send them our way if you’d like to refer a case!), but we do have a soft spot for a real head-scratcher – the kind of case that gets the whole team talking. https://heartvets.co.uk/referral-clinics/refer-a-case/
A recent example is a perfect illustration of when the weird and wonderful bounds into your consult room looking completely normal, only to have you reaching for your textbooks thirty minutes later.
A one-year-old entire male spaniel presented for cardiac investigation following detection of a new, very loud heart murmur during routine clinical examination. This had not been noted when he was examined as a puppy.
The patient was bright and responsive with pink oral mucous membranes and brisk
capillary refill time (<2s). Heart rate was 100bpm with a firm apical impulse, regular rhythm and a radiating grade IV left-sided systolic murmur (PMI apically) and coarse grade II right cranial systolic murmur. Respiratory rate and effort were normal. Abdominal palpation was unremarkable. Femoral pulses were strong and synchronous. Body condition was 4/9 and coat quality was excellent.
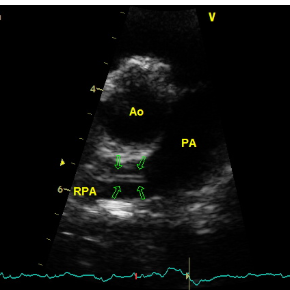
Echocardiography showed the following:
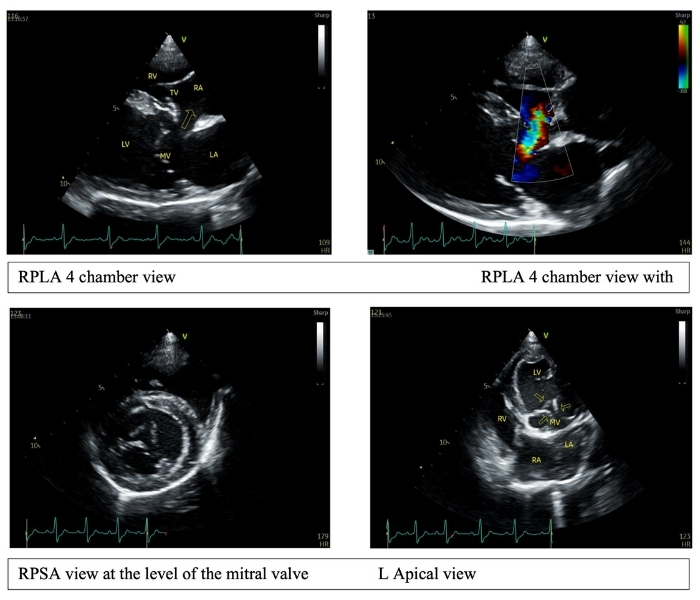
These findings represent an extremely rare group of complex congenital cardiac malformations. With only a handful of cases described in the literature, predicting progression for an individual patient is difficult—particularly as this dog is still so young.
At present, the echocardiographic findings indicate only mild volume loading, with predominantly left-to-right shunting. Over time, we might expect increasing volume loading, and changes in the relative pressures between the chambers could alter the direction of blood flow. This may cause a change in blood flow direction and progressive reduction in systemic oxygenation.
Potential clinical consequences include reduced exercise tolerance, cyanotic episodes, weakness or collapse. Patients may develop left-sided volume overload with signs of left-sided congestive heart failure. Alternatively, reversal of the shunt could result in right-sided congestive heart failure and ascites. As with many structural cardiac abnormalities, there is also a risk of arrhythmia development.
Unfortunately, there is no heroic surgical intervention currently available in veterinary medicine that would meaningfully correct these structural abnormalities.
Given the current findings, and the fact that the patient is clinically well with an excellent quality of life, there is no indication for treatment at this stage. Instead, careful monitoring is the most appropriate approach. We will watch closely for evidence of structural progression and introduce supportive medical management as and when it becomes necessary.
Periodic echocardiography has been recommended, along with packed cell volume (PCV) assessment to monitor for signs of shunt reversal. We also discussed appropriate use of antibiotics in situations where systemic bacteraemia may occur (such as wounds, abscesses or dental disease), as these patients have an increased risk of developing valvular endocarditis.
He may yet live many years, but only time will tell. In the meantime, he continues to enjoy a full and active life, entirely unaware of the extraordinary anatomy he possesses!
Cases like this are a good reminder that not every loud murmur in a young dog follows the textbook. While common conditions account for the majority of findings in practice, occasionally something far more unusual walks through the consulting room door.
For this patient, careful monitoring and a good quality of life are the priorities for now. For clinicians, it highlights the value of keeping an open mind when investigating murmurs in young animals and recognising when referral imaging can reveal something entirely unexpected.
And for those of us who enjoy a good diagnostic puzzle, it is also a reminder of why cardiology never gets boring! We’d love to help with solving any of your cardiac case conundrums!
Recognising and managing heartworm as an emerging risk in travelling and imported dogs

A downloadable client resource to support cardiac patients travelling or being cared for, over the holidays