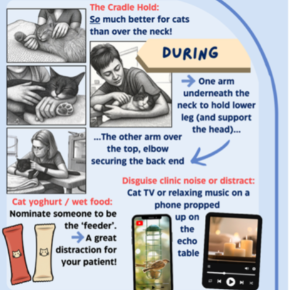
Echo handling hacks for well behaved cats
Surprisingly effective, easy wins to improve the echo experience for your feline patients.

Hypertrophic cardiomyopathy (HCM) and hyperthyroidism are distinct diseases in cats but often partners in disguise. Diagnose one, and the other might be hiding in plain sight. It’s no surprise: both can develop insidiously and share overlapping clinical signs, especially in older patients.
Feline hyperthyroidism can cause secondary cardiac changes that may mimic HCM including myocardial thickening, left atrial enlargement, and hyperdynamic wall motion. These often resolve with treatment, unless underlying cardiac disease is present.
True HCM shows persistent regional or global myocardial thickening, papillary muscle enlargement, and sometimes evidence of outflow tract obstruction. Later changes include diastolic dysfunction, left atrial enlargement, pulmonary oedema, and intracardiac thrombus formation.
It’s not uncommon for cats to have both conditions. Feline hyperthyroidism can unmask or exacerbate cardiac disease, while underlying HCM may go undetected if hyperthyroid signs resolve with treatment. For cats undergoing thyroidectomy or radioactive iodine therapy, cardiac assessment is essential beforehand. Even when owners decline treatment, discussing signs of cardiac disease (and vice versa) is key to early intervention in decompensated cases.
Routine exams may uncover subtle clues, especially in older cats. Obtaining a thorough history is critical. Signs like sleeping more, gradual weight loss, or reduced grooming may be dismissed by owners as normal signs of an older cat. Changes in appetite may not be obvious in multi-cat households, and patient activity may not be noticed if an owner (or the cat!) is out for most of the day.
Clients may be hesitant to pursue diagnostics if their cat does not seem to be “unwell.” A gentle, stepwise approach can help: start with blood pressure and T4 testing; consider adding NT-proBNP to screen for cardiac changes. Though not a perfect test, a raised or abnormal NT-proBNP is a strong indicator for echocardiography. Breed screening is advised in predisposed cats (Maine Coon, British Shorthair, Sphynx) or those with a known family history of cardiac disease. For the feistier feline (often raising your suspicion for hyperthyroidism!) diagnostics can be tricky, especially with the added risk of acute cardiac decompensation. Pre-visit pregabalin or gabapentin (unlicensed) and thoughtful environmental management can go a long way in keeping both patient and team safe.
If CHF is present, stabilise patients before treating feline hyperthyroidism to avoid overloading owners with multiple medications at once. Using gelatin capsules to combine pills can improve compliance at very little cost. If echocardiography isn’t immediately feasible, owner education and regular monitoring is still valuable.
Given the slow progression of both diseases, annual screening is advised to catch emerging pathology – especially in at-risk patients.
Don’t let one diagnosis blind you to the other. These two diseases often walk together – and recognising the overlap can make all the difference in early intervention and outcome. Learn more about how we can help you with your case.
Surprisingly effective, easy wins to improve the echo experience for your feline patients.
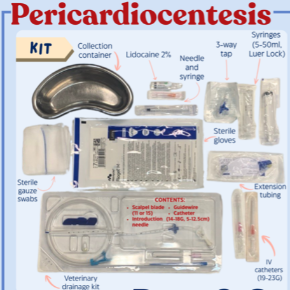
Get ahead and save the stress: our Pericardiocentesis Prep and Go Checklist is the only thing you need!